[[getLangText('background')]]
Gastrointestinal bleeding is a serious complication of coronary artery bypass grafting, and lacks tailored risk assessment tools for personalized interventions. We aimed to develop and validate machine learning algorithms to predict the risk of gastrointestinal bleeding after coronary artery bypass grafting (GIBCG) and to guide its prevention.
Personalized Medicine
1.Precision Intervention for Risk Factors:
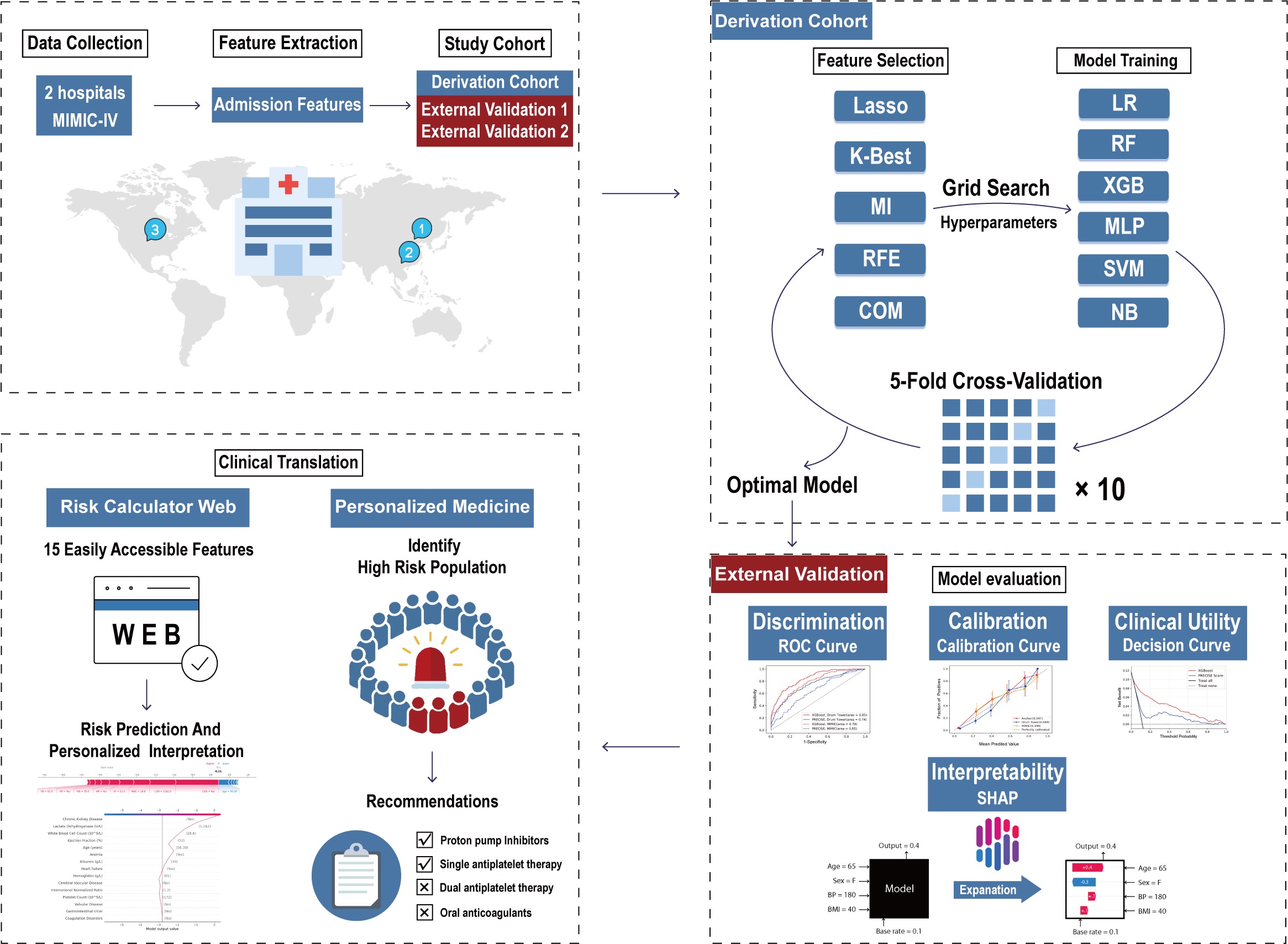
The model provides the patient's GIBCG risk along with prediction interpretations using SHapley Additive exPlanations (SHAP), aiding physicians in understanding the specific impact of each feature on the model's prediction results, which in turn supports medical decision-making.
2.Targeted application of medications:The analysis indicated that preoperative use of proton pump inhibitors (PPIs) and adjustment of antithrombotic agents reduced the incidence of GIBCG in high-risk populations identified by the model, but not in low-risk populations. Therefore, for patients classified as "High Risk," the recommended protocol includes preoperative use of PPIs, careful use of dual antiplatelet therapy (DAPT) and oral anticoagulants (OACs), and consideration of single antiplatelet therapy (SAPT) or alternative antithrombotic treatments. For patients classified as "low risk," it is recommended to confidently administer antiplatelet therapy to those with appropriate indications to reduce the risk of adverse cardiovascular events.
[[getLangText('parameter_description')]]
Age: Age in years.
Chronic comorbidities: Documented in history or met the diagnostic criteria for the following diseases upon admission, including anemia, coagulation disorders, heart failure, cerebrovascular disease, chronic kidney disease, gastrointestinal ulcers, and valvular disease. All listed chronic comorbidities exclude acute onset or diseases that occurred after admission.
Admission examination: Initial laboratory examination results upon admission include white blood cell count (10^9/L), platelet count (10^9/L), hemoglobin (g/L), albumin (g/L), international normalized ratio, and lactate dehydrogenase (U/L). The ejection fraction from the patient’s first echocardiography after admission.
Model name:XGboost
Derivation and validation samples:This multicenter study included patients admitted for surgery during January 2018–June 2022 to Beijing Anzhen Hospital and October 2011–May 2023 to Nanjing Drum Tower Hospital and data from the Medical Information Mart for Intensive Care IV. We developed the model using the Anzhen cohort (n=7,716) and validated it using the Drum Tower (n=2,745) and Medical Information Mart for Intensive Care (n=296) cohorts.
Flowchart:
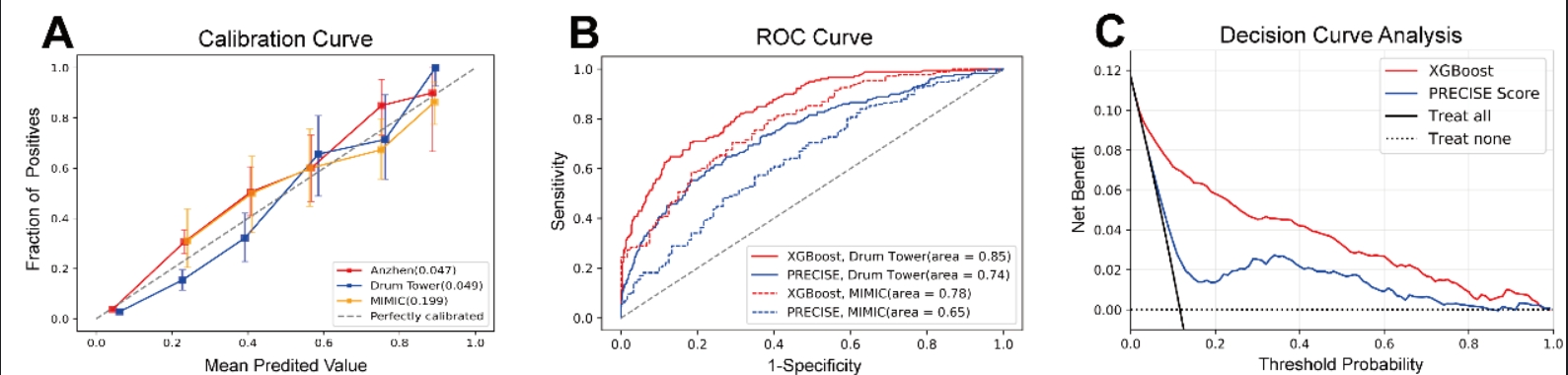
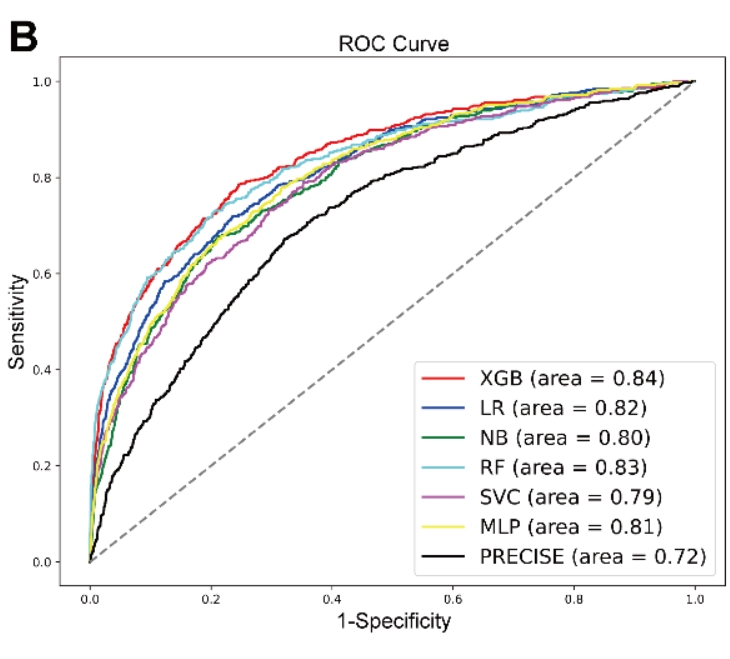
The study process is summarized as follows: data collection from three centers, extraction of patient admission features, and delineation of the study cohort. The Anzhen cohort served as the derivation cohort, used for feature screening and model construction. The optimal model was selected using multiple evaluation metrics and externally validated in the Drum Tower and MIMIC cohorts. Finally, this model was integrated into user-friendly software to facilitate clinical use and guide treatment decisions.
Model Performance:
External Validation: