[[getLangText('background')]]
Esophageal cancer represents a major global health challenge, ranking as the sixth leading cause of cancer-related deaths and accounting for 3.2% of all cancer fatalities annually[1]. In recent years, the incidence has experienced a slight decline.[2].surgical interventions remain common but are often associated with high costs, prolonged recovery, significant trauma, extended hospital stays, and risk of complications. Advances in endoscopic diagnosis and treatment have markedly improved survival rates for early-stage esophageal cancer[3,4].Endoscopic Submucosal Dissection (ESD) is now favored due to its cost-effectiveness, rapid recovery, minimal trauma, and shorter hospital stay[5,6].Current clinical guidelines recommend ESD for T1a esophageal cancer patients without lymph node metastasis and are increasingly including certain T1b patients[7.8]. Japanese guidelines endorse ESD for superficial submucosal cancers (SM1, depth ≤200 μm) when performed by skilled endoscopists[9].Despite these advances, preoperative staging, especially for submucosal tumors, can be inaccurate. Our study found that 6.2% of patients required additional surgical interventions post-ESD due to deeper tumor infiltration than initially diagnosed, causing considerable patient distress. Similar findings have been reported elsewhere, where 23 patients needed esophagectomy after ESD despite clear margins, due to undetected submucosal infiltration[10]. This study aims to develop a diagnostic prediction model employing various methodologies. By analyzing clinical data from patients with early-stage esophageal cancer, the study seeks to improve early treatment strategies, enhance the accuracy of invasion depth assessments, and mitigate the risks associated with both over-treatment and under-treatment.
[[getLangText('parameter_description')]]
PPT:
PCMD:
tumorsize:
esophagealwallthickens:
EOM:
pickledfood:
PLR:
Principle:
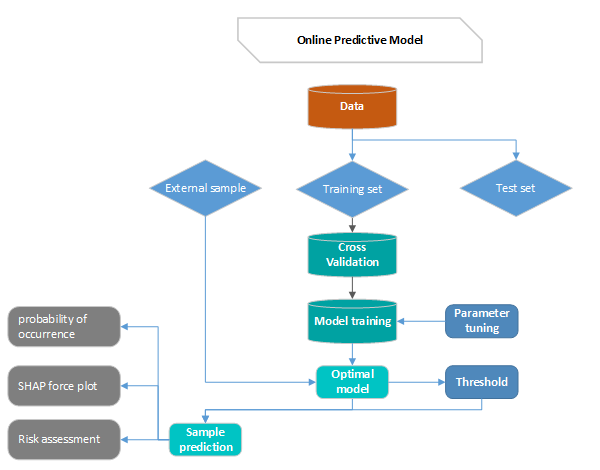
First divide the data into training set and test set, then use the cross-validation method to train the model in the training set, train the optimal model as the final model and record the threshold at this time as the final threshold, and finally observe the model in the test performance on the set. By continuously adjusting the parameters of the model, the generalization ability of the model is improved, and the performance of the model in the training set, validation set and test set is relatively optimal.
By the predicted sample into the optimal model, the model will predict the probability of occurrence, generate the SHAP force plot, and then evaluate the risk according to the predicted probability and prediction.